

Abstract
INTRODUCTION
Anaesthetists may be called upon to emergently secure the airway of a laterally positioned patient. Intubating a patient’s trachea in the lateral position may be difficult due to unfamiliarity. This exploratory study aimed to investigate the success rate of lateral intubation performed by novices in a controlled setting.
METHODS
In this observational study, all patients who presented for elective surgery requiring the lateral position with planned lateral intubation at Singapore General Hospital were included. The trainee assigned to each patient had no prior indication of the proposed lateral intubation until the start of the case. Verbal instructions were given before the start of and during the procedure. The consultant anaesthetist in attendance could intervene at any point to prevent patient harm or if the trainee requested assistance. Time to intubation, adjuncts used and complications encountered were recorded.
RESULTS
A total of 44 consecutive patients were included in this study. The trainees completed 42 of the 44 lateral intubations, with 41 being successfully performed on the first attempt. All patients were intubated successfully in a lateral position within two attempts. The mean duration of intubation was 57.3 ± 36.4 seconds. There was no difference between left and right lateral intubation. Other than one episode of transient desaturation on pulse oximetry, there were no complications.
CONCLUSION
Lateral intubation by trainees had a high success rate when supervised by an experienced operator. Intubation of patients in unconventional positions using routine airway equipment should be included in airway training for trainees.
INTRODUCTION
In the operating theatre, intubation is generally performed with the patient in the supine position. The patient’s position may be changed after the airway has been secured, depending on the surgical requirements. Intubation of patients in the lateral position is unconventional and not routinely performed by most anaesthetic practitioners. It is perceived to be more difficult(1) due to distortion of the airway and the possible need for the operator to adopt an uncomfortable posture. However, in some emergency situations, it may be necessary to secure the airway when the patient is in the lateral position. Various techniques for such a procedure have been studied, some of which involve the use of laryngeal mask airways (LMAs) or lightwands.(2,3)
One of the authors of the present study is a consultant anaesthetist who is experienced in lateral intubation using the Macintosh laryngoscope. As part of his routine anaesthetic practice, he performs and supervises the procedure in the elective setting for patients who require lateral positioning during surgery. Before inducing anaesthesia, the patients are first allowed to find the most comfortable position on their side; this is to minimise pressure injuries and reduce the need for repositioning by operating theatre personnel after the induction of anaesthesia. The present study investigated the success rate of lateral intubation performed by trainees under supervision.
METHODS
This observational study was performed after obtaining approval from the SingHealth Centralised Institutional Review Board, Singapore. The trainee assigned to each case had no prior indication of the proposed lateral intubation until the start of the case. Trainees with no previous experience of lateral intubation were given verbal instructions before the start of the procedure. During the procedure, the consultant could intervene at any point to prevent patient harm or to provide assistance to the trainee, if requested.
All patients who presented for elective surgery requiring the lateral position and had planned lateral intubation at Singapore General Hospital, Singapore, between August 2011 and June 2013 were included in the present study. Patients with unstable cervical spines, previously known difficult intubation and those who required rapid sequence induction were excluded. The patients were informed of the risks of general anaesthesia, including those that result from airway manipulation, as per routine management. They were requested to position themselves in their most comfortable lateral position and a pillow was used to keep their neck in a neutral position. The patient was in the left- or right-sided decubitus position according to the nature of the planned surgery.
Standard monitors including electrocardiography, pulse oximeter, and noninvasive blood pressure, airway pressure, tidal volume and anaesthetic agent monitors were applied. The patient was preoxygenated with oxygen 100% for at least three minutes prior to induction. General anaesthesia was induced using intravenous fentanyl 1–2 mcg/kg and propofol 2–3 mg/kg; atracurium 0.5 mg/kg was used for muscle relaxation. Oral or nasal airways were available if required. After allowing sufficient time for the neuromuscular-blocking drugs to take effect, the anaesthetic trainee would perform intubation using a size 3 Macintosh laryngoscope. A size 4 blade was available if required. For both left and right lateral intubations, the trainee stood at the head end of the patient and held the laryngoscope with his/her left hand; the tracheal tube was inserted using the right hand. If the laryngeal view was inadequate, the backward, upward and rightward pressure (BURP) manoeuvre and/or bougie was used to facilitate intubation.(4) The satisfactory positioning of the tracheal tube was confirmed clinically by auscultation and with the presence of end-tidal carbon dioxide.
Relevant patient details, details on the intubation process, complications encountered and trainees’ perceptions of lateral intubation were recorded. Data was analysed using SPSS version 16.0 (SPSS Inc, Chicago, IL, USA). Categorical data was presented as numbers (percentages) and compared using chi-square test. Continuous variables were presented as mean ± standard deviation (range). Intubation duration between confident and non-confident trainees was compared using Mann-Whitney U test, while trainee confidence levels before and after the intubation attempt were compared using McNemar’s test. A p-value < 0.05 was considered statistically significant.
RESULTS
A total of 44 patients underwent lateral intubation during the study period from August 2011 to June 2013. During preanaesthetic assessment, 2 (4.5%) of the 44 patients were found to have clinical features suggestive of difficult airway. Among the 44 patients, 6 (13.6%) had previous anaesthesia; their modified Cormack and Lehane grades(5) were Grade 1 (n = 2), Grade 2a (n = 3) and Grade 2b (n = 1).
All patients were intubated successfully in the lateral position. Trainees completed 42 of the 44 lateral intubations (i.e. 95.5% trainee success rate). Among the 44 intubations, 41 (93.2%) were successful on the first laryngoscopy attempt. Insertion of the laryngoscope into the oral airway and its removal was considered as one attempt. The mean duration of intubation, defined as the time from the handling of the laryngoscope to the first appearance of end-tidal carbon dioxide tracing, was 57.3 ± 36.4 (range 10–179) seconds. Intubation was achieved within the first minute in 33 (75.0%) of the 44 intubations. Details of the lateral intubations are summarised in
Table I
Characteristics of lateral intubations performed (n = 44).
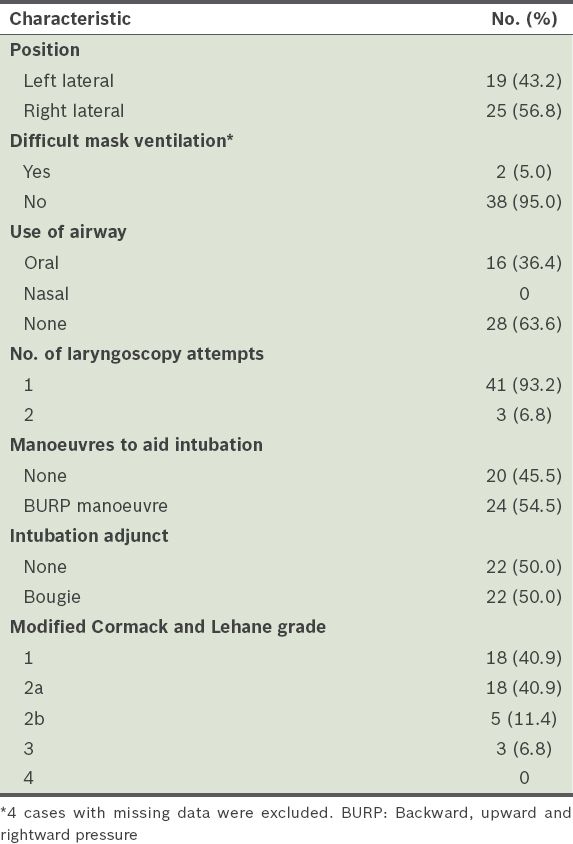
In total, 19 left and 25 right lateral intubations were performed. Although the difference was not statistically significant, more patients intubated in the right lateral position required the BURP manoeuvre to optimise the view of the glottis as compared with patients who were intubated in the left lateral position (n = 16 and n = 8, respectively). Neither left- nor right-sided positioning of the patient appeared to determine satisfactory mask-holding, use of oral airway, Cormack and Lehane classification, number of laryngoscopy attempts or the need for a bougie at intubation.
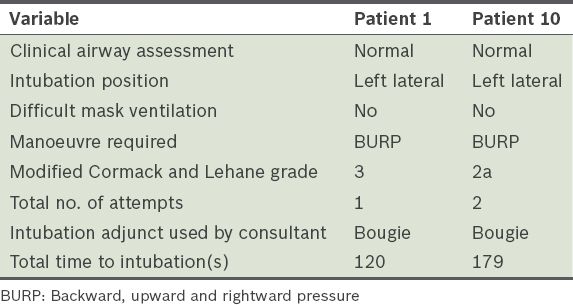
Transient desaturation (below 90%) on pulse oximetry was recorded in a patient (Patient 1) during intubation, requiring intervention from the supervising consultant. Tracheal intubation was achieved without difficulty after adequate bag-mask ventilation and the patient did not suffer further harm. Another tracheal intubation (Patient 10) was performed by the supervising consultant at the trainee’s request due to poor view of the airway (Cormack and Lehane Grade 3). Both of these patients had unremarkable preoperative airway assessments and easy mask ventilation without the need for pharyngeal airway. In these cases, the two trainees had 3.5 and 6 months of prior experience in anaesthesia, respectively; neither of them had prior experience in performing lateral intubations (
Table II
Failed lateral intubation by trainees (n = 2).
The mean duration of the trainees’ anaesthetic experience prior to performing lateral intubation was 24.2 ± 20.5 (range 1.5–96.0) months. 37 (84.1%) of the trainees were medical officers, while 7 (15.9%) were registrars. A significant proportion of the trainees (n = 27, 61.4%) did not have prior experience in lateral intubation. Trainee experience and perception are summarised in
Table III
The experience of the trainees in lateral intubation and their perception of the procedure (n = 44).
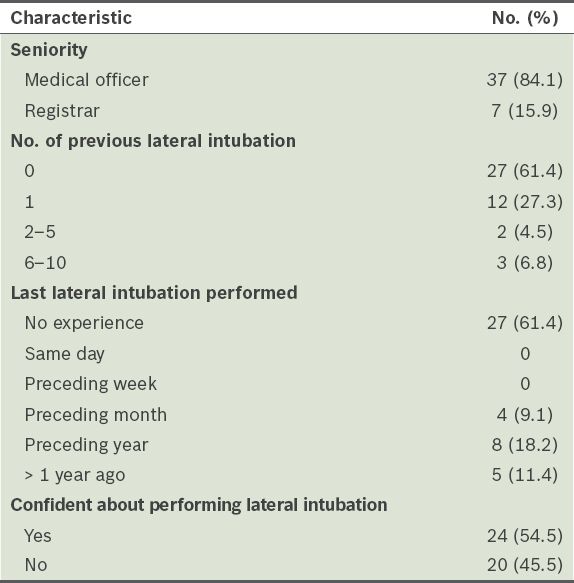
Before attempting the procedure, more trainees were confident about performing lateral intubation (54.5% vs. 45.5%). Trainee confidence did not seem to be related to seniority (i.e. medical officer vs. registrar) or time spent in anaesthetic training; the mean training duration among trainees who were confident was 26.5 ± 17.2 (range 1.5–54.1) months, while the mean training duration among those who did not feel confident was 21.7 ± 23.9 (range 3.0–96.2) months. The mean intubation duration was 46.5 ± 28.1 seconds for the trainees who were confident and 71.1 ± 41.6 seconds for those who were not confident. Although the trend suggested that trainees who were confident were able to secure the airway more quickly, the difference was not statistically significant.
At the end of the procedure, the trainees were asked if they were confident about performing future tracheal intubations for patients in the lateral position. Most of the trainees (n = 33, 75.0%) responded that they were confident about performing lateral intubations after having performed the procedure in a controlled situation (p = 0.004). Nine trainees who were not confident about performing lateral intubation before the case were confident about doing so after performing it successfully under supervision. Among the 44 trainees, 33 (75.0%) stated that they would consider performing lateral intubation in an emergent situation if needed.
DISCUSSION
Lateral intubation is rarely necessary and usually not taught during anaesthetic training. The anatomy of a patient on his/her side may appear unfamiliar to an inexperienced laryngoscopist. Furthermore, performing tracheal intubation when the patient is in the lateral position may force the laryngoscopist to adopt an ergonomically challenging posture. In this preliminary study, we report a high success rate of tracheal intubation in the lateral position among an unselected cohort of anaesthetic trainees, most of whom were new to the technique. The airway was secured in all the patients within two attempts, including three patients with Cormack and Lehane Grade 3 views. The experience in a controlled setting (i.e. with a supervising anaesthetist) resulted in a large proportion of the trainees feeling more confident about performing lateral intubations in the future. Although two trainees were unable to complete the tracheal intubations in the lateral position, we believe that it was the trainees’ relatively short prior experience in airway management rather than the patients’ position that was the main cause of their failure.
There are situations in which performing an intubation with the patient in a lateral position may be advantageous or necessary. Placing a patient with higher risk of regurgitation in a lateral position may mitigate the likelihood of aspiration. It has been suggested that post-tonsillectomy bleeding in a child may be more safely managed with lateral intubation.(6) Emergency intubation may be required for cases in which airway control is accidentally lost during surgery in the lateral position. It may be too painful or impractical to reposition a patient who has posterior injuries or foreign bodies lodged in his/her back. Rapid control of the airway in these situations is imperative as delays in achieving adequate oxygenation may be catastrophic. Acquiring an additional set of intubation skills using basic equipment such as the Macintosh laryngoscope or a bougie is always useful, especially when more sophisticated airway tools are unavailable.
Nathanson et al used manikins to evaluate the performance of trainees in lateral intubation and demonstrated that intubation in the left lateral position was more time-consuming and difficult than intubation in the supine position.(1) However, they also found that intubation success improved with practice, indicating a learning curve.(1) In other words, prior training in lateral intubation is likely to improve the success rate, should the technique be required in an emergency. Intuitively, intubation in the left lateral position may be easier than intubation in the right lateral position, as patients’ tongues tend to fall to the left in the former position, affording an easier view of the glottis. However, apart from the trend of needing to perform the BURP manoeuvre more frequently among patients who were intubated in the right lateral position, we did not find either position to be easier or quicker in the present study. This may have been due to the relatively small numbers of trainees included.
McCaul et al found that the left lateral position deteriorated laryngoscopic views in 35% of their patients when compared to the supine position.(7) The study also reported a dissociation between the quality of the laryngoscopic view and ease of tracheal intubation, as well as a lower rate of intubation success (79.5%) as compared to the present study.(7) The better intubation rate in the present study could be due to the fact that a bougie was used when performing lateral intubations even if the glottis could be partially visualised (half of the patients in the present study were intubated with the aid of a bougie). McCaul et al suggested that LMA insertion during lateral intubation could have resulted in a higher success rate and more rapid control of the airway.(7) However, if there was an increased risk of aspiration or the LMA was a poor fit, more definitive control using an endotracheal tube may be preferred.
Other methods of securing the airway in the lateral position have been described. Biswas et al and Komatsu et al performed lateral intubation on 82 and 50 patients, respectively, by first inserting an intubating LMA to guide blind tracheal intubation.(3,8) The first-time success rates of these two studies, after optimising LMA position, were 86.6% and 82%, respectively, while the overall success rates were 98.8% and 96%, respectively.(3,8) Dimitriou et al similarly compared left and right lateral intubation using an intubating LMA, with the addition of a flexible lightwand that was inserted into the tracheal tube to guide intubation.(2) The first left and right lateral intubation success rates were 90% and 95%, respectively, with an eventual success rate of 100%.(2)
Despite the high rate of success, the use of an intubating LMA is known to take longer than direct laryngoscopy in supine patients for intubation.(9) The possible increased risk of regurgitation and aspiration from the longer intubation process and ventilation through the LMA is unknown. In addition, as intubation via an LMA is a blind-on-blind technique, it may not be an intuitive first-choice technique in an emergency situation. We would argue that as most anaesthetists are experienced with intubation via direct laryngoscopy, albeit usually in the supine position, the use of direct laryngoscopy in lateral intubation would likely be an easier next step than the use of an intubating LMA.
Further studies involving a larger sample size, which can involve seasoned practitioners, may give a more reliable estimate of the success rate of lateral intubation. As the purpose of the present study was to demonstrate the feasibility of instructing trainees on the technique of intubating a patient in the lateral position, the design and sample size precluded its ability to address less common complications of airway manipulation or the ability to ventilate with a face mask. Future studies should include patient anthropometric data, details of airway assessment and the haemodynamic effects of intubation.
To conclude, the present study showed that intubation in the lateral position has a high success rate when performed by a novice operator under supervision. Anaesthetists should be well-versed in the technique for use in an emergency situation. We recommend making tracheal intubation in the lateral position part of airway management training.
ACKNOWLEDGEMENT
We thank Dr Sui An Lie, Department of Anaesthesiology, Singapore General Hospital, Singapore, for her assistance in data collection in the present study.