Prognostic factors for mortality due to pneumonia among adults from different age groups in Singapore and mortality predictions based on PSI and CURB-65
Singapore Med J 2018; 59(4): 190-198 doi: https://doi.org/10.11622/smedj.2017079
Prognostic factors for mortality due to pneumonia among adults from different age groups in Singapore and mortality predictions based on PSI and CURB-65
Zoe Xiaozhu Zhang1, MBBS, PhD, Yang Yong2,3, MBBS, PhD, Wan C Tan4, MD, FRCP, Liang Shen5, PhD, Han Seong Ng6, MD, Kok Yong Fong3, MD
Author Information >Copyright and License information >
1Department of Clinical Epidemiology, Tan Tock Seng Hospital, Singapore 2Department of Epidemiology, Singapore General Hospital, Singapore 3Medical Board, Singapore General Hospital, Singapore 4UBC James Hogg Research Centre, Heart Lung Institute, St Paul’s Hospital, Canada 5Biostatistics Unit, NUS Yong Loo Lin School of Medicine, National University Health System, Singapore 6CEO Office, Singapore General Hospital, Singapore Correspondence: Dr Zoe Zhang Xiaozhu, Senior Epidemiologist, Department of Clinical Epidemiology, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore 308433. zoe_zhang_xz@ttsh.com.sg
Pneumonia is associated with considerable mortality. However, there is limited information on age-specific prognostic factors for death from pneumonia.
METHODS
Patients hospitalised with a diagnosis of pneumonia through the emergency department were stratified into three age groups: 18–64 years, 65–84 years and ≥ 85 years. Multivariate logistic regression and receiver operating characteristic curve analyses were conducted to evaluate prognostic factors for mortality and the performance of pneumonia severity scoring tools for mortality prediction.
RESULTS
A total of 1,902 patients were enrolled (18–64 years: 614 [32.3%]; 65–84 years: 944 [49.6%]; ≥ 85 years: 344 [18.1%]). Mortality rates increased with age (18–64 years: 7.3%; 65–84 years: 16.1%; ≥ 85 years: 29.7%; p < 0.001). Malignancy and tachycardia were prognostic of mortality among patients aged 18–64 years. Male gender, malignancy, congestive heart failure and eight other parameters reflecting acute disease severity were associated with mortality among patients aged 65–84 years. For patients aged ≥ 85 years, altered mental status, tachycardia, blood urea nitrogen, hypoxaemia, arterial pH and pleural effusion were significantly predictive of mortality. The Pneumonia Severity Index (PSI) was more sensitive than CURB-65 (confusion, uraemia, respiratory rate ≥ 30 per minute, low blood pressure, age ≥ 65 years) for mortality prediction across all age groups.
CONCLUSION
The predictive effect of prognostic factors for mortality varied among patients with pneumonia from the different age groups. PSI performed significantly better than CURB-65 for mortality prediction, but its discriminative power decreased with advancing age.
Community-acquired pneumonia (CAP), the most common infectious disease worldwide, is associated with considerable morbidity and mortality. It has a particularly high incidence and mortality rate among elderly people.(1-7) Young and middle-aged patients (aged < 65 years) die from CAP as well, although the incidence rate is low.(8,9) Many studies have examined the predictive risk factors of CAP mortality in adults.(10-13) Increasing age, male gender, comorbidities and multilobar consolidation are often of prognostic significance.(14-17) However, patients of different ages have distinct physiological characteristics, clinical presentations and treatment responses, and therefore age group-specific prognostic factors of mortality may be more useful for the clinical management of pneumonia.
The Pneumonia Severity Index (PSI) and CURB-65 (confusion, uraemia, respiratory rate ≥ 30 per minute, low blood pressure, age ≥ 65 years) are the most commonly used clinical scoring tools for severity assessment and mortality prediction of pneumonia.(10,18-23) Higher scores generally suggest more severe diseases and higher risk of death. The performance of these severity scoring tools, however, varies among subsets of patients of different ages. Underestimation of the risk of death with increasing age has often been reported.(24-26)
Pneumonia represents a significant healthcare issue in Singapore. It is the fifth most common cause of hospitalisation and the second principal cause of death.(27) In 2014, pneumonia was the underlying cause that was responsible for approximately 19% of all deaths reported in the country.(28) In the present study, we retrospectively analysed all admitted patients with CAP from three age groups (ages 18–64 years, 65–84 years and ≥ 85 years) to identify prognostic factors for mortality when they presented to the emergency department (ED). We also evaluated the performance of PSI and CURB-65 for mortality prediction among patients with CAP in Singapore.
METHODS
The study was performed at Singapore General Hospital, Singapore, a large tertiary hospital with more than 1,500 beds. All patients admitted to the hospital after presenting to the ED with a primary diagnosis of pneumonia between 1 January 2012 and 31 December 2013 were included for chart review. Patients were considered to have a primary diagnosis of pneumonia if they had an ICD-9-CM (International Classification of Diseases, 9th revision, Clinical Modification) code of 480.x to 487.x. Patients were stratified into three age groups: 18–64 years, 65–84 years and ≥ 85 years. Ethical approval and waiver of informed consent was obtained from the SingHealth Centralised Institutional Review Board (2014/226/A). This study was funded by the SingHealth Foundation Research Grant (SHF/FG590S/2013). The 30-day mortality data was provided by the National Registry of Disease Office, Health Promotion Board, Singapore.
Pneumonia was defined as an acute infection of the lung parenchyma that is characterised by symptoms of acute respiratory infection and the presence of an acute pulmonary infiltrate on chest radiography or abnormal auscultatory findings.(29) Patients who had human immunodeficiency virus infection, pulmonary tuberculosis or cystic fibrosis, or those on long-term immunosuppressant or steroid treatment were excluded, in view that these diseases entailed varying progression, clinical management and prognosis.
A total of 27 prognostic factors were evaluated. Among them, 20 variables were derived from the PSI scoring tool developed by Fine et al,(10) including demographic factors (e.g. age and gender), comorbidities (e.g. malignancy, renal disease, liver disease, cerebrovascular disease and congestive heart disease), initial vital signs (e.g. altered mental status [AMS], temperature, pulse rate, respiratory rate and systolic blood pressure), laboratory test results (e.g. levels of blood urea nitrogen [BUN], blood glucose, serum sodium, haematocrit, blood oxygen and arterial pH) and chest radiography findings (e.g. pleural effusion). In addition, eight other common chronic illnesses in the Singapore local population were evaluated, including ischaemic heart disease, chronic obstructive pulmonary disease, diabetes mellitus, hypertension, asthma, bronchiectasis, Parkinson’s disease and dementia.(30) Data on initial vital signs, laboratory test results and chest radiography findings were from the first readings taken in the ED.
The indices of PSI and CURB-65 were calculated according to the original studies.(10,19) The primary outcome was all-cause mortality at 30 days after admission to the hospital. Data on intensive care unit admission and hospital length of stay was also recorded. Categorical variables were expressed as counts (percentage). Continuous variables were expressed as mean ± standard deviation or median with 25th–75th interquartile range (IQR).
Differences in frequencies were compared using chi-square test. Mann-Whitney U test or Kruskal-Wallis test was used to assess any differences in continuous variables that were not normally distributed. To evaluate the potential prognostic factors associated with mortality, univariate analysis was first performed using the chi-square test. Factors with p < 0.05 were included into the multivariate logistic regression model. The goodness-of-fit was tested using Hosmer-Lemeshow goodness-of-fit test. Odds ratios (ORs) and 95% confidence intervals (CIs) were presented. Factors with event frequency < 1.5% were excluded from the analysis. Standard sensitivity, specificity, positive predictive value and negative predictive value were calculated at various cut-offs for the PSI and CURB-65 scores. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the discriminatory power of PSI and CURB-65 for mortality prediction. Area under the curve (AUC) with 95% CI was computed for each age group of patients. All statistical tests were two-tailed and p < 0.05 was considered to be statistically significant. All analyses were performed using IBM SPSS Statistics version 20 for Windows (IBM Corp, Armonk, NY, USA).
RESULTS
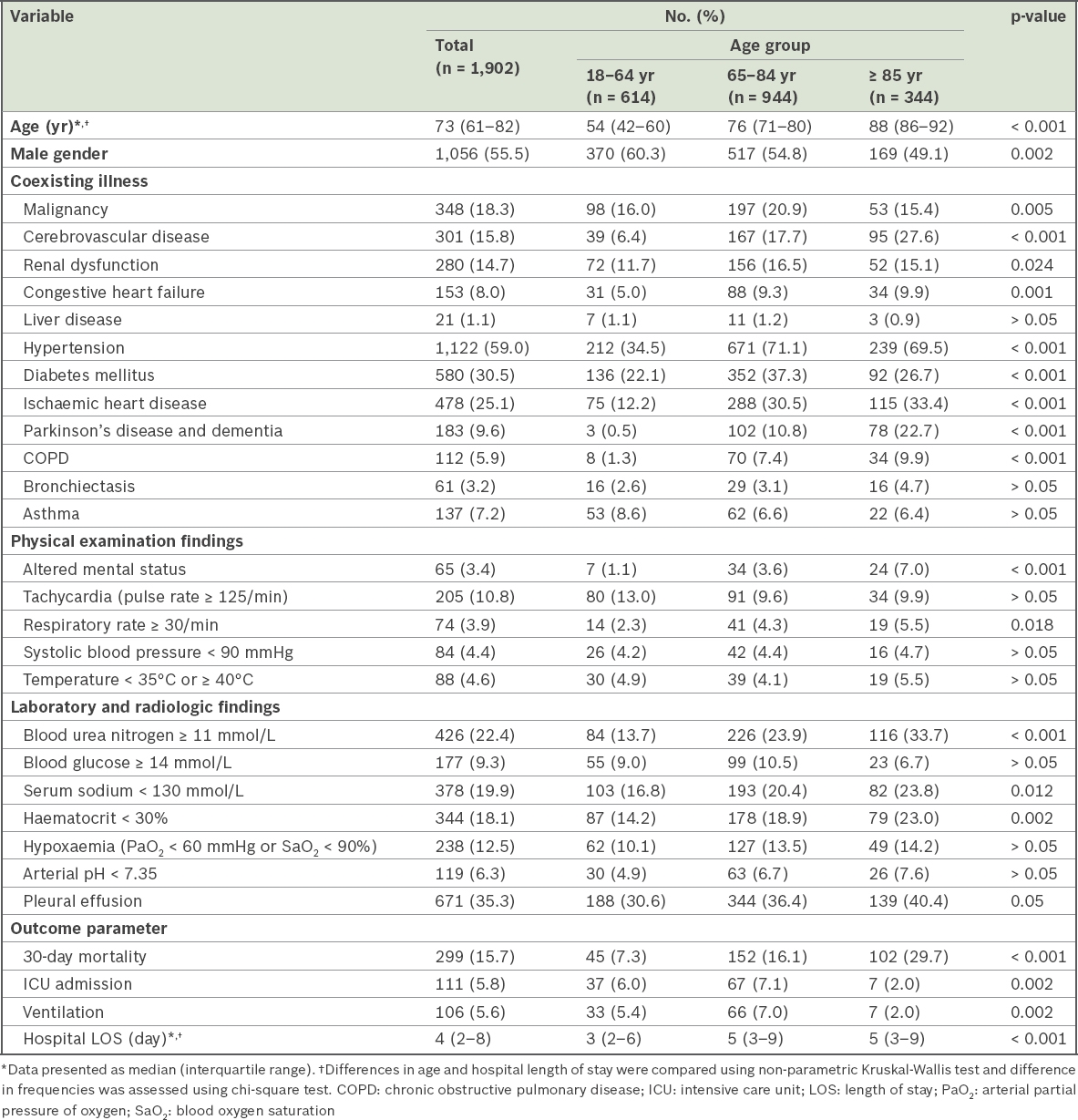
Baseline characteristics and clinical outcomes of patients across the three age groups are summarised in Table I. A total of 1,902 patients satisfied the study criteria, including 614 (32.3%) patients aged 18–64 years, 944 (49.6%) patients aged 65–84 years and 344 (18.1%) patients aged ≥ 85 years. The overall 30-day mortality rate was 15.7% (n = 299), comprising 85.3% in-hospital deaths and 14.7% post-discharge deaths. Individual mortality rates for the three age groups were 7.3%, 16.1% and 29.7%, respectively, for patients aged 18–64 years, 65–84 years and ≥ 85 years (p < 0.001). Most of the evaluated comorbidities were less common among younger patients (aged 18–64 years), but had similar prevalence among patients aged 65–84 years and ≥ 85 years. Liver disease was rare in our cohort (1.1%). In terms of clinical presentation and laboratory test results, patients aged 65–84 years and ≥ 85 years more frequently had AMS, respiratory rate ≥ 30/minute, and abnormal BUN, serum sodium and haematocrit levels at the time of ED admission. They also stayed significantly longer in hospital. The younger patients more frequently presented with tachycardia (pulse rate ≥ 125/minute).
Table I
Baseline characteristics and clinical outcomes of patients with community-acquired pneumonia.
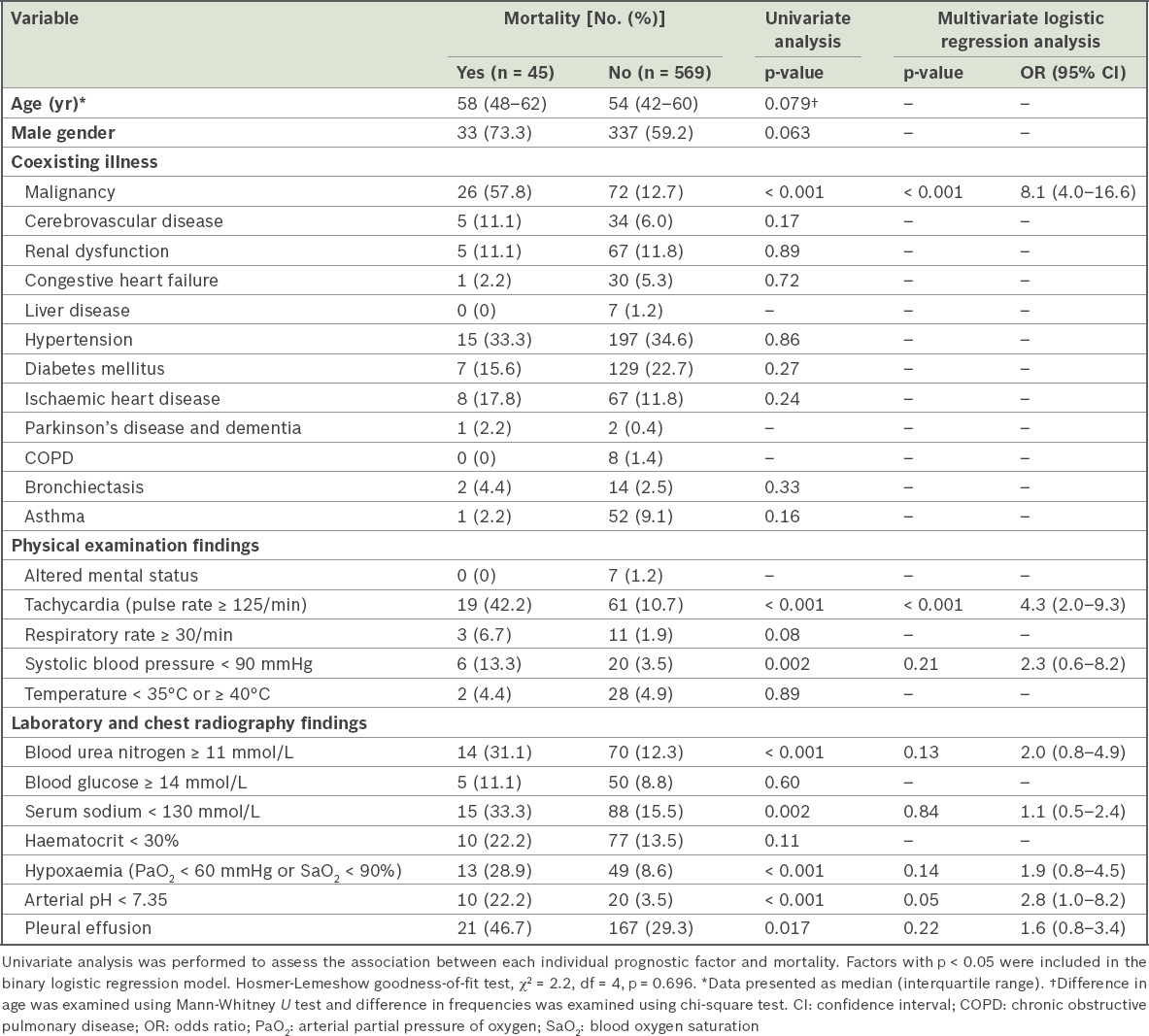
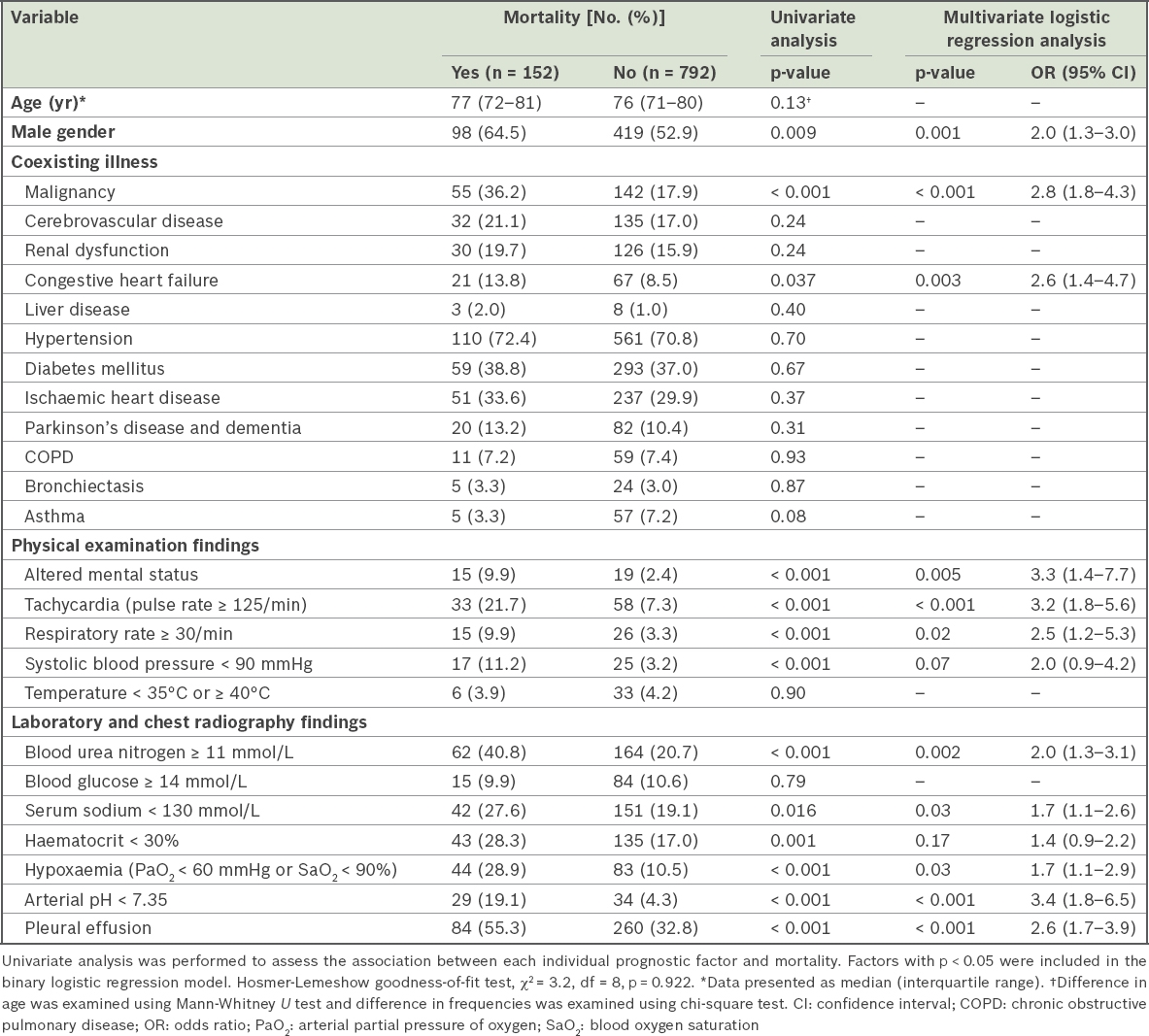
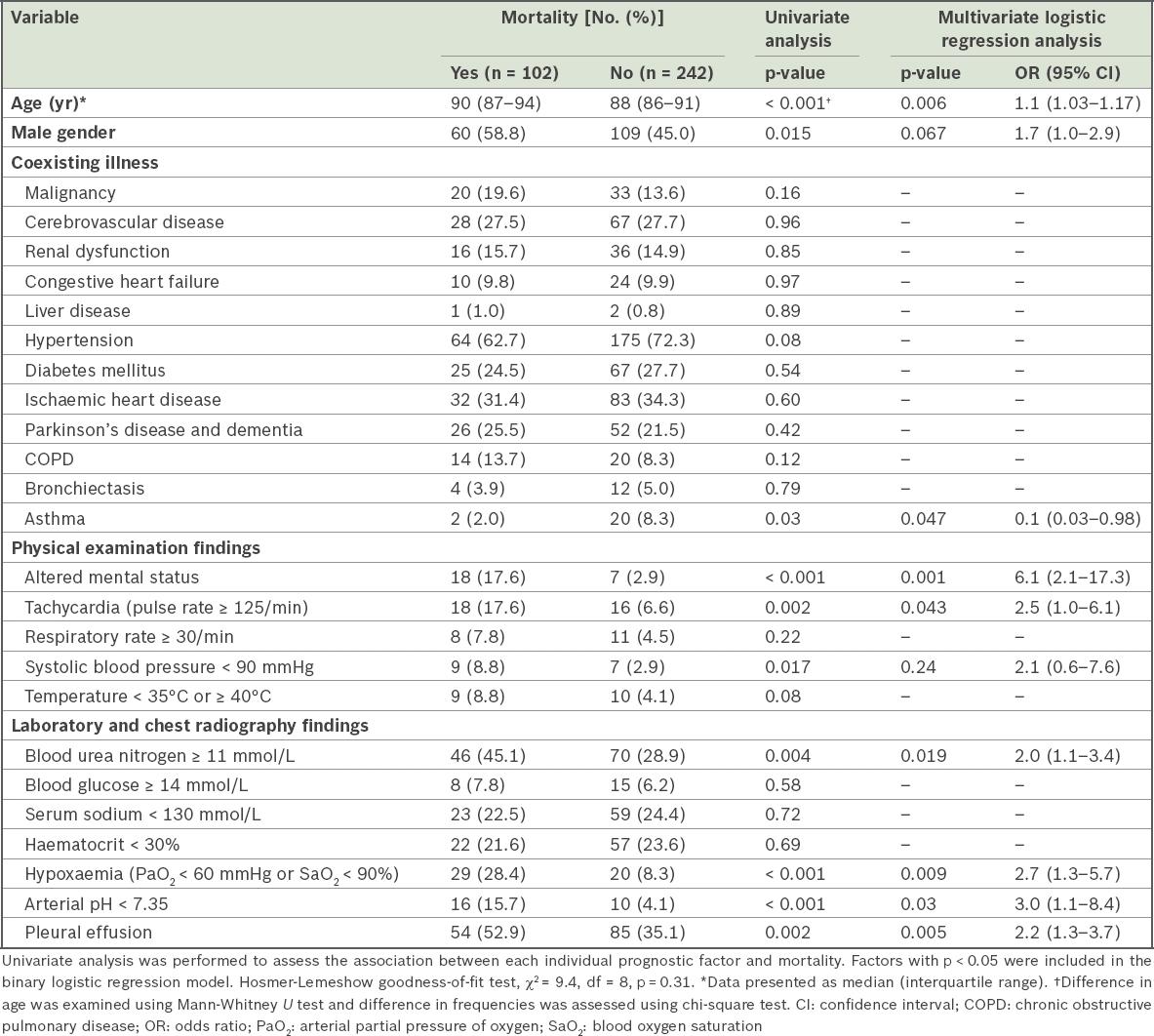
The association between prognostic factors and mortality were evaluated among the three age groups of patients (Tables II–IV). For patients aged 18–64 years, liver disease, Parkinson’s disease and dementia, chronic obstructive pulmonary disease and AMS were excluded from the analysis because of low event frequencies. Eight factors with p < 0.05 on univariate analysis were included in the multivariate logistic regression model. Malignancy and tachycardia showed an independent association with mortality, with ORs of 8.1 (IQR 4.0–16.6) and 4.3 (IQR 2.0–9.3), respectively (Table II). Among patients aged 65–84 years, 13 factors had p < 0.05 on the chi-square test and were subsequently included in the multivariate logistic regression analysis. 11 of these factors showed a significant association with mortality, including male gender, malignancy, congestive heart failure, AMS, tachycardia, respiratory rate ≥ 30 per minute, BUN ≥ 11 mmol/L, serum sodium < 130 mmol/L, hypoxaemia, arterial pH < 7.35 and pleural effusion (Table III). AMS (OR 3.3, 95% CI 1.4–7.7), tachycardia (OR 3.2, 95% CI 1.8–5.6) and arterial pH < 7.35 (OR 3.4, 95% CI 1.8–6.5) ranked among the top three factors showing a significant association with mortality. Among patients aged ≥ 85 years, no comorbidities significantly increased the risk of death (Table IV). Asthma, however, showed a negative association with mortality among this group of patients (OR 0.1, 95% CI 0.03–0.98; p = 0.047). Age, AMS (OR 6.1, 95% CI 2.1–17.3), tachycardia, BUN ≥ 11 mmol/L, hypoxaemia, arterial pH < 7.35 and pleural effusion were independently associated with mortality in the final multivariate logistic regression analysis.
Table II
Association of prognostic factors with mortality among patients with pneumonia aged 18–64 years (n = 614).
Table III
Association of risk factors with mortality among patients with pneumonia aged 65–84 years (n = 944).
Table IV
Association of risk factors with mortality among patients with pneumonia aged ≥ 85 years (n = 344).
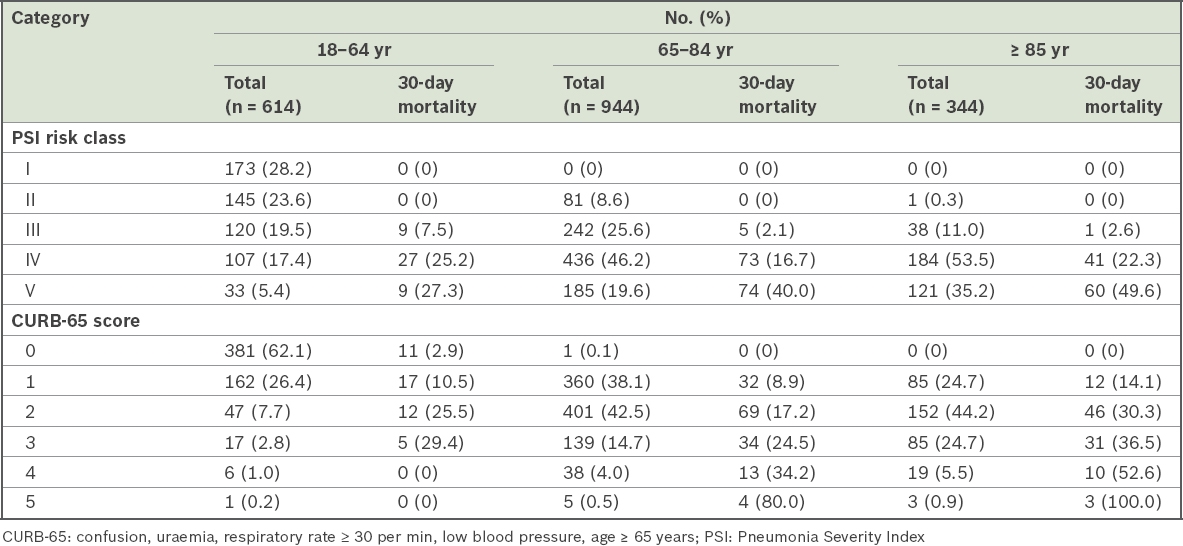
Table V
Mortality in PSI and CURB-65 severity classes among different age groups.
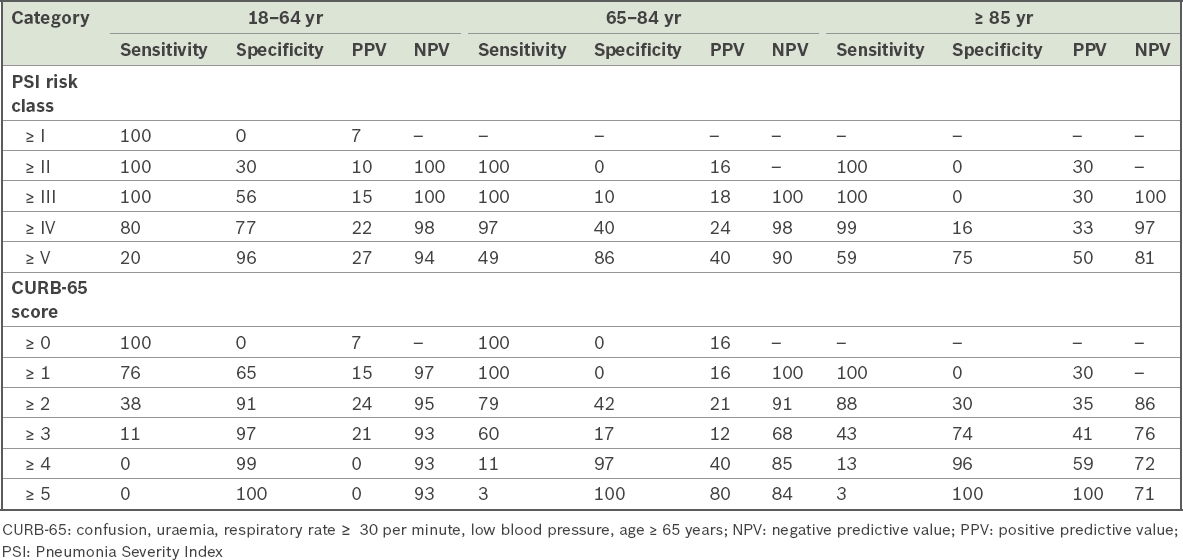
Table VI
Sensitivity, specificity, positive predictive value and negative predictive value for the prediction of 30-day mortality at different cut-offs of PSI and CURB-65.
When patients were stratified into different severity classes according to PSI and CURB-65 scores, the mortality rates increased significantly with increasing severity levels (Table V). However, the 30-day mortality of PSI Class III among patients aged 18–64 years was significantly higher than that in the other two age groups (18–64 years: 7.5%; 65–84 years: 2.1%; ≥ 85 years: 2.6%, p < 0.001). Patients with CURB-65 score 1 had 30-day mortality rates in the range 8.9%–14.1%.
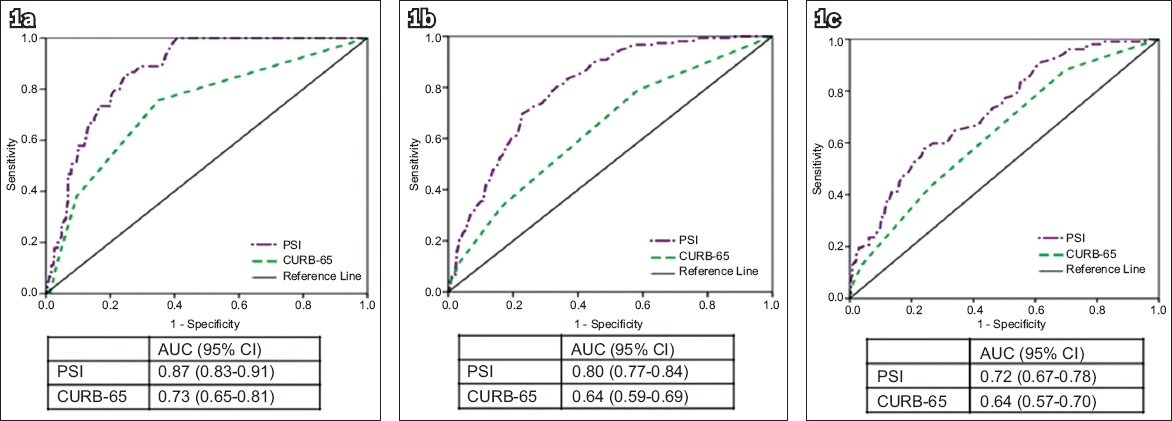
The sensitivity, specificity, positive predictive value and negative predictive value of PSI and CURB-65 for predicting 30-day mortality for each age group are shown in Table VI. In general, PSI was more sensitive than CURB-65 for mortality prediction among patients with CAP. Among patients aged 18–64 years, the sensitivity of PSI had a big drop from 100% to 80% at the Class IV cut-off, whereas it remained at 97% and 99%, respectively, in the other two patient groups. ROC curve analysis revealed a trend of decreasing accuracy in relation to higher age categories for both PSI and CURB-65 (Fig. 1). The AUC of PSI appeared higher than that of CURB-65 in each age group.
Fig. 1
Receiver operating characteristic curves show PSI and CURB-65 with respect to prediction of 30-day mortality for patients with pneumonia aged (a) 18–64 years, (b) 65–84 years and (c) ≥ 85 years. AUC: area under the curve; CI: confidence interval; CURB-65: confusion, uraemia, respiratory rate ≥ 30 per minute, low blood pressure, age ≥ 65 years; PSI: Pneumonia Severity Index
DISCUSSION
In this study, we defined predictive risk factors for mortality in three age-specific groups of patients with pneumonia in Singapore. Among patients aged 18–64 years, malignancy and tachycardia (pulse rate ≥ 125 per minute) were significantly associated with mortality. A total of 11 factors were prognostic for mortality among patients aged 65–84 years, including malignancy, congestive heart failure, male gender and eight other parameters reflecting initial vital signs and abnormal laboratory results. For patients aged ≥ 85 years, age, initial vital signs and abnormal laboratory test results were critical for mortality prediction.
Increasing age has been defined as a predictive factor for mortality in pneumonia patients in many studies, especially among patients aged 65 years or older.(10,19,31) In our study, age significantly increased the risk of death only among patients aged ≥ 85 years. Conte et al, who analysed more than 2,000 patients aged ≥ 65 years, suggested that age ≥ 85 years was an independent predictive factor for mortality.(32) Calle et al reported that age ≥ 90 years was markedly associated with mortality.(33) Ageing is associated with a progressively weakened immune system and decreased lung performance. For patients of extreme age (≥ 85 years in our study), these changes alone are probably drastic, which independently increases the risk of death due to pneumonia.
Comorbid condition is another well-recognised risk factor for death due to pneumonia.(8,34) Fine et al have defined the significant prognostic value of five types of chronic illnesses as per PSI among patients of all ages, including malignancy, liver disease, renal disease, congestive heart failure and cerebrovascular disease.(10) Marrie et al studied over 11,000 Canadian patients aged 18–55 years and depicted a similar spectrum of chronic illnesses associated with pneumonia death.(34) Among the 13 comorbidities evaluated in this study, only malignancy and congestive heart failure were significantly predictive of mortality among patients aged 18–64 years and/or 65–84 years. Most of the chronic diseases studied were common among patients aged ≥ 85 years. However, none were independently associated with greater mortality. It is known that the prognosis of a disease in elderly people is often determined by the patient’s overall health status.(14,35,36) It is very likely that coexisting chronic diseases work in a synergic manner, affecting patients’ general health condition and increasing the severity of disease and the mortality rate, although they are not independently associated with death. We also noticed the increasing trend of malignancy, Parkinson’s disease and dementia, and chronic obstructive pulmonary disease among the non-survivors aged ≥ 85 years in our study. A study with a larger sample size would give a more definite conclusion.
In particular, asthma showed a negative association with mortality among patients with pneumonia aged ≥ 85 years. Asthma is a known risk factor of pneumonia.(37) Asthmatic patients with CAP have been reported to present earlier to the hospital, are more often given antibiotic treatment before hospital admission, and generally have low CAP severity.(38,39) All these may indicate that these patients are more aware of respiratory problems, even when symptoms are mild, and actively seek medical care earlier during the course of disease. In contrast, non-asthmatic elderly patients may not be aware of the symptoms of CAP as early as asthmatics, causing a subsequent delay in diagnosis, admission and treatment, thus resulting in higher mortality.
Initial vital signs and the results of basic laboratory tests and chest radiography are critical information that is required for clinicians to rapidly understand patients’ health condition, in particular the severity of acute illness and how well the body copes with it. In this study, AMS, increased BUN, hypoxaemia and pleural effusion were significantly associated with mortality among patients aged 65–84 years and ≥ 85 years, which was consistent with the findings of Fine et al.(10) The non-survivors among patients aged 18–64 years also more frequently had increased BUN, hypoxaemia and pleural effusion, but the difference did not reach statistical significance.
Young patients rarely presented with AMS. However, AMS appeared to be a strong predictor for mortality among the two older patient groups, increasing the risk of death by 3.3 and 6.1 times, respectively. Infection has been reported as one of the commonest causes for AMS in the ED. One in nine elderly patients presenting with AMS are reported to die during their hospital stay.(40) Therefore, timely diagnosis and intervention is critical. Accurate assessment, however, can be challenging when the change of mental status is subtle and the patients are very elderly.(41)
Tachycardia and acidosis (arterial pH < 7.35) were independently associated with mortality among all three patient groups. Although tachycardia is usually a nonspecific clinical presentation that can be influenced by many factors, it is associated with the severity of pneumonia and often appears ahead of other severe clinical presentations.(10,42,43) Physicians probably need to be alert to the occurrence of tachycardia in patients with pneumonia, and close monitoring and aggressive clinical management may be necessary. Acidosis is usually associated with central nervous system malfunctions, with patients likely to become disoriented or comatose; therefore, acute treatment is critical.
PSI and CURB-65 are the most well-validated risk prediction models of CAP. PSI performs better than CURB-65 among patients in Singapore.(44) In our study, PSI was more accurate than CURB-65 for severity stratification. However, it was worth noting that PSI Class III, which was defined as a low-risk class of death in the original study,(10) unexpectedly had a mortality rate of 7.5% among patients aged 18–64 years in our study. Other researchers have also reported that PSI could incorrectly categorise young patients with severe pneumonia into low-risk classes due to the inappropriate weight accorded to age.(25,45) The ROC analysis in our study revealed that the best PSI cut-off score for mortality prediction was about 85–90 for younger patients, which was equivalent to PSI Class III (data not shown). Therefore, taking PSI Class III as a low-risk class of death may not be appropriate for the younger patient groups. On the contrary, elderly patients in the low PSI severity classes would most likely survive within 30 days of admission. This was demonstrated in a recent study conducted among a group of patients with healthcare-associated pneumonia and a median age of 80 years.(46) As to mortality prediction, PSI showed higher sensitivity than CURB-65 for every age group. However, its power of discrimination decreased with advancing age. Chen et al have reported similar findings and believed that the excessive weight given to a patient’s age leads to overestimation of disease severity among elderly patients with pneumonia.(25)
High hospital admission rate and high mortality rate are the two major characteristics of CAP in Singapore.(44) In our study, over 85% of death among patients with pneumonia occurred in hospital. Therefore, the medical care these patients receive in hospital is one of the critical factors that is closely associated with their final clinical outcome. As the prognostic factors evaluated here are all readily available when patients visit EDs, clear awareness of these factors and understanding of their predictive value would help physicians to predict the clinical outcome and customise the medical care being provided. For younger patients aged 18–64 years, malignancy stood out as a strong predictive factor for mortality, as it increased the odds of death by 8.1 times. These findings suggest that close monitoring and intensive clinical intervention are most likely indispensable, even if the PSI severity level is not high. For patients aged ≥ 85 years, severity in the acute phase of the disease was strongly associated with mortality. Elderly patients with pneumonia may clinically present only with delirium or acute confusion instead of respiratory signs or symptoms. However, a change of mental state is critical in forecasting the high risk of death not long after. Physicians probably need to explain and discuss the potential adverse outcome with family members while tailoring medical treatment and clinical management strategies.
This study had several limitations. First, it had a retrospective design. We extracted pre-existing data from patients’ case notes, which might not be as accurate as data collected prospectively by means of direct interview or questionnaire. Second, we were unable to assess the variables that were not available in the medical records, even though they might have been important to the study. Third, our study may have been underpowered with regard to the detection of some associations due to the inadequacy of sample size for subgroup analyses.
In conclusion, the risk factors for mortality in pneumonia patients were not the same across different age groups. PSI was more accurate for mortality prediction than CURB-65. However, its discriminative power decreased with advancing age among patients with pneumonia.
ACKNOWLEDGEMENTS
We are grateful for the diligent work done by Ms Michelle Liu Ping, Research Coordinator, Department of Epidemiology, Medical Board, Singapore General Hospital, in the process of patient case note review.
References Jackson ML, Nelson JC, Jackson LA.Risk factors for community-acquired pneumonia in immunocompetent seniors.J Am Geriatr Soc. 2009;57:882-8. Koivula I, Stén M, Mäkelä PH.Prognosis after community-acquired pneumonia in the elderly:a population-based 12-year follow-up study.Arch Intern Med. 1999;159:1550-5. Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia.JAMA. 1997;278:2080-4. Marrie TJ, Haldane EV, Faulkner RS, Durant H, Kwan C.Community-acquired pneumonia requiring hospitalization. Is it different in the elderly?.J Am Geriatr Soc. 1985;33:671-80. Riquelme R, Torres A, El-Ebiary M, et al. Community-acquired pneumonia in the elderly:a multivariate analysis of risk and prognostic factors.Am J Respir Crit Care Med. 1996;154:1450-5. Venkatesan P, Gladman J, Macfarlane JT, et al. A hospital study of community acquired pneumonia in the elderly.Thorax. 1990;45:254-8. Cillóniz C, Polverino E, Ewig S, et al. Impact of age and comorbidity on cause and outcome in community-acquired pneumonia.Chest. 2013;144:999-1007. Simpson JC, Macfarlane JT, Watson J, Woodhead MA.A national confidential enquiry into community acquired pneumonia deaths in young adults in England and Wales. British Thoracic Society Research Committee and Public Health Laboratory Service.Thorax. 2000;55:1040-5. Trotter CL, Stuart JM, George R, Miller E.Increasing hospital admissions for pneumonia, England.Emerg Infect Dis. 2008;14:727-33. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia.N Engl J Med. 1997;336:243-50. Farr BM, Sloman AJ, Fisch MJ.Predicting death in patients hospitalized for community-acquired pneumonia.Ann Intern Med. 1991;115:428-36. Fine MJ, Orloff JJ, Arisumi D, et al. Prognosis of patients hospitalized with community-acquired pneumonia.Am J Med. 1990;88:1N-8N. Fine MJ, Smith MA, Carson CA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis.JAMA. 1996;275:134-41. Marrie TJ, Wu L.Factors influencing in-hospital mortality in community-acquired pneumonia:a prospective study of patients not initially admitted to the ICU.Chest. 2005;127:1260-70. Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia:results from the Pneumonia Patient Outcomes Research Team cohort study.Arch Intern Med. 2002;162:1059-64. Metersky ML, Waterer G, Nsa W, Bratzler DW.Predictors of in-hospital vs postdischarge mortality in pneumonia.Chest. 2012;142:476-81. Wilson PA, Ferguson J.Severe community-acquired pneumonia:an Australian perspective.Intern Med J. 2005;35:699-705. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia.Am J Med. 2005;118:384-92. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital:an international derivation and validation study.Thorax. 2003;58:377-82. Huang DT, Weissfeld LA, Kellum JA, et al. Risk prediction with procalcitonin and clinical rules in community-acquired pneumonia.Ann Emerg Med. 2008;52:48-58.e2. Capelastegui A, España PP, Quintana JM, et al. Validation of a predictive rule for the management of community-acquired pneumonia.Eur Respir J. 2006;27:151-7. Man SY, Lee N, Ip M, et al. Prospective comparison of three predictive rules for assessing severity of community-acquired pneumonia in Hong Kong.Thorax. 2007;62:348-53. Menéndez R, Martinez R, Reyes S, et al. Biomarkers improve mortality prediction by prognostic scales in community-acquired pneumonia.Thorax. 2009;64:587-91. Parsonage M, Nathwani D, Davey P, Barlow G.Evaluation of the performance of CURB-65 with increasing age.Clin Microbiol Infect. 2009;15:858-64. Chen JH, Chang SS, Liu JJ, et al. Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects.Thorax. 2010;65:971-7. Mody L, Sun R, Bradley S.Community-acquired pneumonia in older veterans:does the pneumonia prognosis index help?.J Am Geriatr Soc. 2002;50:434-8. Ministry of Health Singapore. Top 10 Conditions of Hospitalisation 2015. Available at: https://www.moh.gov.sg/content/moh_web/home/statistics/Health_Facts_Singapore/Top_10_Conditions_of_Hospitalisation.html. Accessed February 5 2016. Ministry of Health Singapore. Principal causes of death 2015. Available from: https://www.moh.gov.sg/content/moh_web/home/statistics/Health_Facts_Singapore/Principal_Causes_of_Death.html. Accessed February 5 2016. Bartlett JG, Dowell SF, Mandell LA, et al. Practice guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases Society of America.Clin Infect Dis. 2000;31:347-82. Health Promotion Board, SingaporeChronic Disease Management 2015. Available from: http://www.hpb.gov.sg/HOPPortal/health-article/HPBSUEXTAPP1_4022097. Accessed February 12 2016. Sligl WI, Each DT, Marrie TJ, Majumdar SR.Age still matters:prognosticating short- and long-term mortality for critically ill patients with pneumonia.Crit Care Med. 2010;38:2126-32. Conte HA, Chen YT, Mehal W, Scinto JD, Quagliarello VJ.A prognostic rule for elderly patients admitted with community-acquired pneumonia.Am J Med. 1999;106:20-8. Calle A, Márquez MA, Arellano M, et al. Geriatric assessment and prognostic factors of mortality in very elderly patients with community-acquired pneumonia.Arch Bronconeumol. 2014;50:429-34. Marrie TJ, Carriere KC, Jin Y, Johnson DH.Factors associated with death among adults <55 years of age hospitalized for community-acquired pneumonia.Clin Infect Dis. 2003;36:413-21. Ewig S, Kleinfeld T, Bauer T, et al. Comparative validation of prognostic rules for community-acquired pneumonia in an elderly population.Eur Respir J. 1999;14:370-5. Torres OH, Muñoz J, Ruiz D, et al. Outcome predictors of pneumonia in elderly patients:importance of functional assessment.J Am Geriatr Soc. 2004;52:1603-9. Marrie TJ.Community-acquired pneumonia in the elderly.Clin Infect Dis. 2000;31:1066-78. Terraneo S, Polverino E, Cilloniz C, et al. Severity and outcomes of community acquired pneumonia in asthmatic patients.Respir Med. 2014;108:1713-22. Liapikou A, Bakali D, Pantazopoulos I, et al. Community acquired pneumonia in asthma patients.Eur Respir J. 2013;42:P2720. Leong LB, Jian KH, Vasu A, Seow E.Prospective study of patients with altered mental status:clinical features and outcome.Int J Emerg Med. 2008;1:179-82. Janssens JP, Krause KH.Pneumonia in the very old.Lancet Infect Dis. 2004;4:112-24. Corrales-Medina VF, Musher DM, Wells GA, et al. Cardiac complications in patients with community-acquired pneumonia:incidence, timing, risk factors, and association with short-term mortality.Circulation. 2012;125:773-81. McFadden JP, Price RC, Eastwood HD, Briggs RS.Raised respiratory rate in elderly patients:a valuable physical sign.Br Med J (Clin Res Ed). 1982;284:626-7. Zhang ZX, Zhang W, Liu P, et al. Prognostic value of Pneumonia Severity Index, CURB-65, CRB-65, and procalcitonin in community-acquired pneumonia in Singapore.Proceedings of Singapore Healthcare. 2015;25:139-47. Schuetz P, Koller M, Christ-Crain M, et al. Predicting mortality with pneumonia severity scores:importance of model recalibration to local settings.Epidemiol Infect. 2008;136:1628-37. Abisheganaden J, Ding YY, Chong WF, et al. Health-care associated pneumonia (HCAP):identification of low and high-risk patients.Current Respiratory Medicine Reviews. 2015;11:241-6.
REFERENCES:
1. Jackson ML, Nelson JC, Jackson LA. Risk factors for community-acquired pneumonia in immunocompetent seniors. J Am Geriatr Soc 2009; 57:882-8. https://doi.org/10.1111/j.1532-5415.2009.02223.x
PMid:19453307
2. Koivula I, Stén M, Mäkelä PH. Prognosis after community-acquired pneumonia in the elderly: a population-based 12-year follow-up study. Arch Intern Med 1999; 159:1550-5. https://doi.org/10.1001/archinte.159.14.1550
PMid:10421277
3. Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA 1997; 278:2080-4. https://doi.org/10.1001/jama.1997.03550230056037
PMid:9403422
4. Marrie TJ, Haldane EV, Faulkner RS, Durant H, Kwan C. Community-acquired pneumonia requiring hospitalization. Is it different in the elderly? J Am Geriatr Soc 1985; 33:671-80. https://doi.org/10.1111/j.1532-5415.1985.tb01775.x
PMid:4045084
5. Riquelme R, Torres A, El-Ebiary M, et al. Community-acquired pneumonia in the elderly: a multivariate analysis of risk and prognostic factors. Am J Respir Crit Care Med 1996; 154:1450-5. https://doi.org/10.1164/ajrccm.154.5.8912763
PMid:8912763
6. Venkatesan P, Gladman J, Macfarlane JT, et al. A hospital study of community acquired pneumonia in the elderly. Thorax 1990; 45:254-8. https://doi.org/10.1136/thx.45.4.254
PMid:2356552 PMCid:PMC473766
7. Cillóniz C, Polverino E, Ewig S, et al. Impact of age and comorbidity on cause and outcome in community-acquired pneumonia. Chest 2013; 144:999-1007. https://doi.org/10.1378/chest.13-0062
PMid:23670047
8. Simpson JC, Macfarlane JT, Watson J, Woodhead MA. A national confidential enquiry into community acquired pneumonia deaths in young adults in England and Wales. British Thoracic Society Research Committee and Public Health Laboratory Service. Thorax 2000; 55:1040-5. https://doi.org/10.1136/thorax.55.12.1040
PMid:11083890 PMCid:PMC1745667
9. Trotter CL, Stuart JM, George R, Miller E. Increasing hospital admissions for pneumonia, England. Emerg Infect Dis 2008; 14:727-33. https://doi.org/10.3201/eid1405.071011
PMid:18439353 PMCid:PMC2600241
10. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997; 336:243-50. https://doi.org/10.1056/NEJM199701233360402
PMid:8995086
11. Farr BM, Sloman AJ, Fisch MJ. Predicting death in patients hospitalized for community-acquired pneumonia. Ann Intern Med 1991; 115:428-36. https://doi.org/10.7326/0003-4819-115-6-428
PMid:1872491
12. Fine MJ, Orloff JJ, Arisumi D, et al. Prognosis of patients hospitalized with community-acquired pneumonia. Am J Med 1990; 88:1N-8N.
PMid:2195886
13. Fine MJ, Smith MA, Carson CA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA 1996; 275:134-41. https://doi.org/10.1001/jama.1996.03530260048030
PMid:8531309
14. Marrie TJ, Wu L. Factors influencing in-hospital mortality in community-acquired pneumonia: a prospective study of patients not initially admitted to the ICU. Chest 2005; 127:1260-70. https://doi.org/10.1378/chest.127.4.1260
15. Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 2002; 162:1059-64. https://doi.org/10.1001/archinte.162.9.1059
PMid:11996618
16. Metersky ML, Waterer G, Nsa W, Bratzler DW. Predictors of in-hospital vs postdischarge mortality in pneumonia. Chest 2012; 142:476-81. https://doi.org/10.1378/chest.11-2393
PMid:22383662
18. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med 2005; 118:384-92. https://doi.org/10.1016/j.amjmed.2005.01.006
PMid:15808136
19. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003; 58:377-82. https://doi.org/10.1136/thorax.58.5.377
PMid:12728155 PMCid:PMC1746657
20. Huang DT, Weissfeld LA, Kellum JA, et al. Risk prediction with procalcitonin and clinical rules in community-acquired pneumonia. Ann Emerg Med 2008; 52:48-58 e2.
21. Capelastegui A, Espa-a PP, Quintana JM, et al. Validation of a predictive rule for the management of community-acquired pneumonia. Eur Respir J 2006; 27:151-7. https://doi.org/10.1183/09031936.06.00062505
PMid:16387948
22. Man SY, Lee N, Ip M, et al. Prospective comparison of three predictive rules for assessing severity of community-acquired pneumonia in Hong Kong. Thorax 2007; 62:348-53. https://doi.org/10.1136/thx.2006.069740
PMid:17121867 PMCid:PMC2092476
23. Menéndez R, Martinez R, Reyes S, et al. Biomarkers improve mortality prediction by prognostic scales in community-acquired pneumonia. Thorax 2009; 64:587-91. https://doi.org/10.1136/thx.2008.105312
PMid:19131448
24. Parsonage M, Nathwani D, Davey P, Barlow G. Evaluation of the performance of CURB-65 with increasing age. Clin Microbiol Infect 2009; 15:858-64. https://doi.org/10.1111/j.1469-0691.2009.02908.x
PMid:19702590
25. Chen JH, Chang SS, Liu JJ, et al. Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects. Thorax 2010; 65:971-7. https://doi.org/10.1136/thx.2009.129627
PMid:20965934
26. Mody L, Sun R, Bradley S. Community-acquired pneumonia in older veterans: does the pneumonia prognosis index help? J Am Geriatr Soc 2002; 50:434-8. https://doi.org/10.1046/j.1532-5415.2002.50107.x
PMid:11943037
29. Bartlett JG, Dowell SF, Mandell LA, et al. Practice guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis 2000; 31:347-82. https://doi.org/10.1086/313954
PMid:10987697
31. Sligl WI, Eurich DT, Marrie TJ, Majumdar SR. Age still matters: prognosticating short- and long-term mortality for critically ill patients with pneumonia. Crit Care Med 2010; 38:2126-32. https://doi.org/10.1097/CCM.0b013e3181eedaeb
PMid:20818232
32. Conte HA, Chen YT, Mehal W, Scinto JD, Quagliarello VJ. A prognostic rule for elderly patients admitted with community-acquired pneumonia. Am J Med 1999; 106:20-8. https://doi.org/10.1016/S0002-9343(98)00369-6
33. Calle A, Márquez MA, Arellano M, et al. Geriatric assessment and prognostic factors of mortality in very elderly patients with community-acquired pneumonia. Arch Bronconeumol 2014; 50:429-34. https://doi.org/10.1016/j.arbres.2014.01.012
PMid:24629763
34. Marrie TJ, Carriere KC, Jin Y, Johnson DH. Factors associated with death among adults < 55 years of age hospitalized for community-acquired pneumonia. Clin Infect Dis 2003; 36:413-21. https://doi.org/10.1086/346037
PMid:12567298
35. Ewig S, Kleinfeld T, Bauer T, et al. Comparative validation of prognostic rules for community-acquired pneumonia in an elderly population. Eur Respir J 1999; 14:370-5. https://doi.org/10.1183/09031936.99.14237099
PMid:10515416
36. Torres OH, Mu-oz J, Ruiz D, et al. Outcome predictors of pneumonia in elderly patients: importance of functional assessment. J Am Geriatr Soc 2004; 52:1603-9. https://doi.org/10.1111/j.1532-5415.2004.52492.x
PMid:15450034
37. Marrie TJ. Community-acquired pneumonia in the elderly. Clin Infect Dis 2000; 31:1066-78. https://doi.org/10.1086/318124
PMid:11049791
38. Terraneo S, Polverino E, Cilloniz C, et al. Severity and outcomes of community acquired pneumonia in asthmatic patients. Respir Med 2014; 108:1713-22. https://doi.org/10.1016/j.rmed.2014.09.001
PMid:25245791
39. Liapikou A, Bakali D, Pantazopoulos I, et al. Community acquired pneumonia in asthma patients. Eur Respir J 2013; 42:P2720.
40. Leong LB, Jian KH, Vasu A, Seow E. Prospective study of patients with altered mental status: clinical features and outcome. Int J Emerg Med 2008; 1:179-82. https://doi.org/10.1007/s12245-008-0049-8
PMid:19384512 PMCid:PMC2657274
42. Corrales-Medina VF, Musher DM, Wells GA, et al. Cardiac complications in patients with community-acquired pneumonia: incidence, timing, risk factors, and association with short-term mortality. Circulation 2012; 125:773-81. https://doi.org/10.1161/CIRCULATIONAHA.111.040766
PMid:22219349
43. McFadden JP, Price RC, Eastwood HD, Briggs RS. Raised respiratory rate in elderly patients: a valuable physical sign. Br Med J (Clin Res Ed) 1982; 284:626-7. https://doi.org/10.1136/bmj.284.6316.626
44. Zhang ZX, Zhang W, Liu P, et al. Prognostic value of Pneumonia Severity Index, CURB-65, CRB-65, and procalcitonin in community-acquired pneumonia in Singapore. Proceedings of Singapore Healthcare 2015; 25:139-47. https://doi.org/10.1177/2010105815623292
45. Schuetz P, Koller M, Christ-Crain M, et al. Predicting mortality with pneumonia severity scores: importance of model recalibration to local settings. Epidemiol Infect 2008; 136:1628-37. https://doi.org/10.1017/S0950268808000435
PMid:18302806 PMCid:PMC2870789
46. Abisheganaden J, Ding YY, Chong WF, et al. Health-care associated pneumonia (HCAP): identification of low and high-risk patients. Current Respiratory Medicine Reviews 2015; 11:241-6. https://doi.org/10.2174/1573398X11666150928194824