

Abstract
INTRODUCTION
Tuberculosis (TB), a potentially fatal infectious disease, poses significant health problems. The objective of this study was to analyse trends among newly diagnosed TB patients seen at the Singapore General Hospital (SGH).
METHODS
This study was a retrospective case record review of notified TB patients at SGH between 2006 and 2010 (inclusive).
RESULTS
A total of 1,979 cases of TB were notified over the five years. The number increased from 368 in 2006 to 407 in 2010 (p = 0.51), in tandem with the increasing number of patients seen at the hospital and the rising population in Singapore. Singaporean residents accounted for 82.8% of the cases, while non-Singaporean residents and non-residents made up the remainder. The year-to-year percentage of non-Singaporean residents and non-residents notified remained stable throughout the five years (p = 0.783). The number of male Singaporean residents (70.7%) notified was more than twice that of female Singaporean residents (29.3%). The majority of patients infected with TB (31.9%) were elderly patients aged > 65 years. Although testing for the human immunodeficiency virus increased from 43.8% (2006) to 64.2% (2010), the number detected with coinfection remained stable (14 and 12 patients in 2006 and 2010, respectively). Mortality rates also remained stable at 12.0%.
CONCLUSION
We cannot afford complacency, as there was no downward trend in the number of notified TB cases at SGH from 2006 to 2010. As the elderly contribute significantly to the TB burden, increased efforts are required to manage this vulnerable population.
INTRODUCTION
Tuberculosis (TB) is a potentially fatal infectious disease caused by the Mycobacterium tuberculosis bacterium. Despite the availability of effective drug treatments, TB remains an international health problem and is the second leading cause of death from an infectious disease after human immunodeficiency virus (HIV) infection.(1) In 2012, an estimated 8.6 million people developed TB and 1.3 million died from the disease; Southeast Asian countries accounted for 29% of the TB cases worldwide.(1) Although Singapore has the lowest incidence of TB (41.5 cases per 100,000 population of residents and long-stayers) among the Southeast Asian countries,(2) TB control continues to remain a challenge.(3) For this reason, our study aimed to analyse trends among newly diagnosed TB patients who were seen at the Singapore General Hospital (SGH).
METHODS
The case records of all patients with TB notified at SGH from 2006 to 2010 were retrospectively reviewed. TB incidence and patient demographics were compared on a yearly basis and analysed using IBM SPSS Statistics version 21.0 (IBM Corp, Armonk, NY, USA). Study approval was obtained from the SingHealth Centralised Institutional Review Board C.
RESULTS
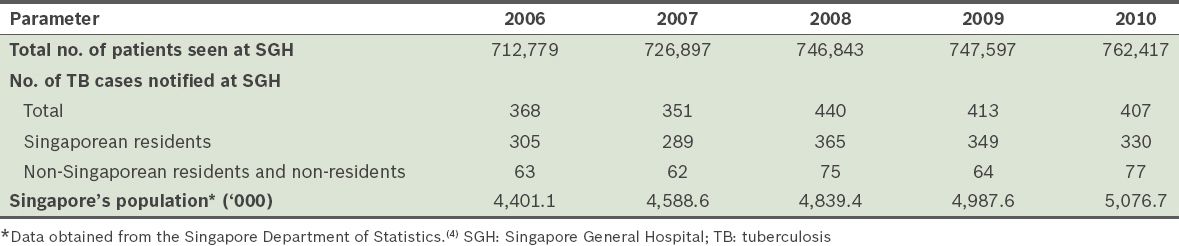
A total of 1,979 cases of TB were notified at SGH over the five years. In tandem with the increasing number of patients seen at SGH and the rising population in Singapore, the number of patients notified to have TB increased from 368 cases in 2006 to 407 cases in 2010 (
Table I
Total number of patients seen and cases of TB notified at SGH, and Singapore’s population between 2006 and 2010.
Among the Singaporean residents notified to have TB at SGH, 77.1% were Chinese, 14.6% were Malay, 6.0% were Indian and 2.3% were of other races. Male Singaporean residents (70.7%) made up more than twice the number of cases as compared to female Singaporean residents (29.3%). In contrast, the gender distribution was almost equal (46.0% men; 54.0% women) among the non-Singaporean residents and non-residents who were notified to have TB at SGH (
Fig. 1
Bar graph shows the distribution of patients with tuberculosis according to their gender and residency status (n = 1,979).
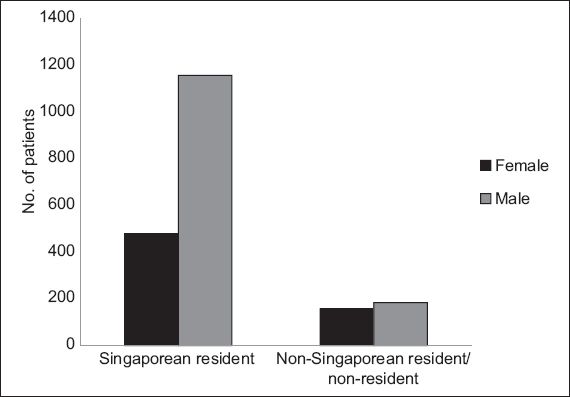
Fig. 2
Bar graph shows the distribution of patients with tuberculosis (TB) according to their age groups and year of TB notification.
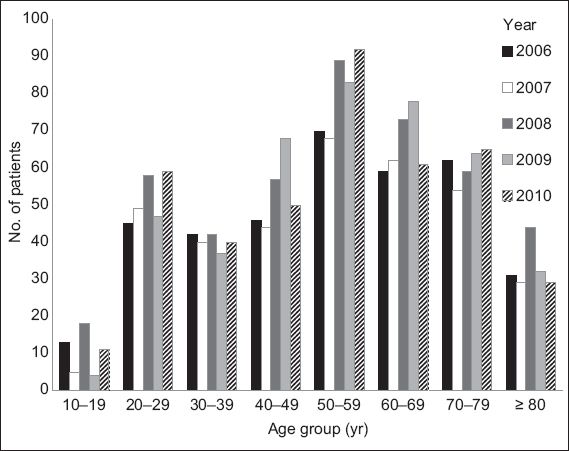
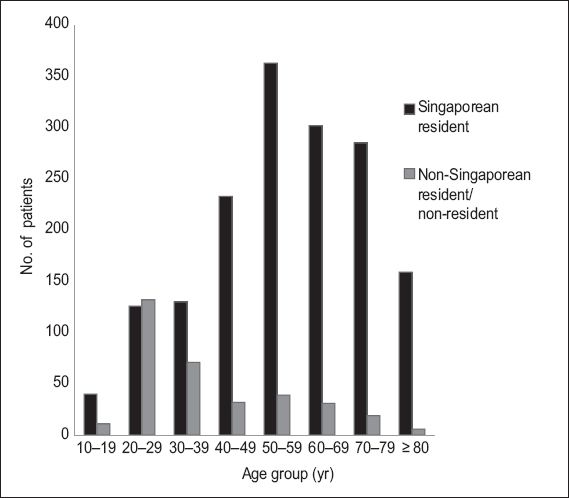
Fig. 3
Bar graph shows the distribution of patients with tuberculosis according to their age and residency status.
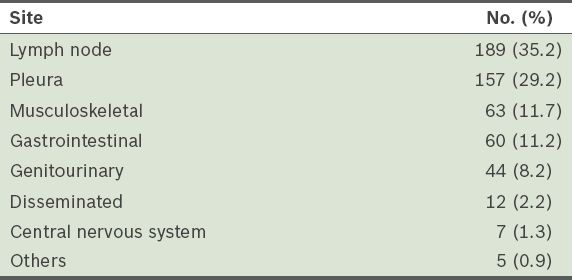
Extrapulmonary TB was diagnosed in 537 of the 1,979 cases (27.1%), at the sites shown in
Table II
Sites of extrapulmonary tuberculosis (n = 537).
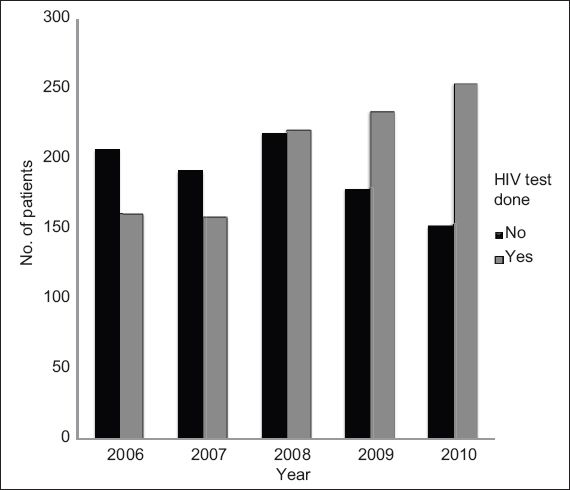
HIV testing of patients who were newly diagnosed with TB showed an upward trend from 43.8% in 2006 to 64.2% in 2010 (
Fig. 4
Bar graph shows the distribution of patients who had HIV tests done in the years 2006–2010.
Among the 1,979 cases of TB notified, 44.5% were treated at SGH, while the care of 29.8% was transferred to other health institutions and 8.9% left the country. The diagnosis of TB was revised for 89 (4.5%) patients – 86 patients were found to have nontuberculous mycobacteria, one patient had granulomatous inflammation from a lymph node biopsy but cultures for TB and clinical examination were negative, and the last two patients who were initially clinically diagnosed with TB did not show temporal response to treatment.
The overall mortality rate was 12.0% and remained stable throughout the five years; 28 (1.4%) patients died from TB, while the remaining 210 (10.6%) patients died from other causes, mainly cancer, pneumonia, ischaemic heart disease and sepsis. Among the patients who died from TB, the mean age was 59.7 ± 22.5 years, 67.9% were male, 75.0% were smear positive for acid fast bacilli and 17.9% were immunocompromised (two patients were HIV positive, two were on immunosuppressive agents for rheumatological conditions and one was on chemotherapy for cancer). Among these 28 patients, 16 had fulminant pulmonary TB, eight had disseminated TB, two had massive haemoptysis and two had TB meningitis. 22 out of the 28 patients (78.6%) were diagnosed at their first presentation to the hospital, while the remaining 6 (21.4%) patients were diagnosed at a median of 1.5 (range 1–6) months after presentation to the hospital (the delay in diagnosis was due to confounding medical illnesses). Of the 28 patients, 10 (35.7%) died in the intensive care unit.
DISCUSSION
SGH is a tertiary care referral centre that services specific geographic parts of Singapore. It also has busy haematology, oncology, rheumatology and transplant units that care for a large population of immunocompromised patients. Although SGH accounts for approximately 20% of the TB notifications in Singapore,(2) the patient profiles obtained in the present study may not be reflective of TB patients in Singapore as a whole.
Despite the efforts made to control TB, we did not observe a downward trend in the number of TB patients notified at SGH from 2006 to 2010. Similarly, from 2011 to 2013, the number of TB patients notified at SGH did not change significantly – 383, 436 and 373 cases in 2011, 2012 and 2013, respectively. Medical tourism and the high influx of foreign workers were postulated to contribute to the increased number of TB cases seen in Singapore.(3) However, this was not reflected in the present study, where the percentage of non-Singaporean residents and non-resident cases notified remained stable over the five years (p = 0.783).
We did not find any racial predilection for TB infection. While the racial distribution of TB cases notified at SGH was proportional to Singapore’s racial distribution,(4) the racial distribution of TB cases in Singapore (as reported by the Ministry of Health, Singapore) showed that Malays had the highest incidence of TB.(2) Our study found that male Singaporean residents accounted for more than twice the number of TB cases as compared to female Singaporean residents; this concurs with the ministry’s data, which stated that male patients made up 64.0% of new TB cases notified in Singapore.(2) However, this gender disparity was not seen among the non-Singaporean residents and non-residents – the higher representation of women in this group could be due to the large number of foreign domestic workers. The higher percentage of TB cases notified in Singapore among non-Singaporean residents and non-residents within the 20–29 years age group is also likely to be related to the foreign worker population. Additional stringent screenings should perhaps be mandated as part of their pre-employment screening.
In Singapore, 9.0% of the population comprises elderly persons (i.e. aged > 65 years).(4) In the present study, we found that most (31.9%) of the patients notified to have TB at SGH were elderly. This is similar to the percentages reported for Singapore(2) and other developed countries; the elderly accounted for 36.9% of the annual TB notifications in Hong Kong(5) and 20% in the United States.(6) The higher risk of TB among the elderly was ascribed to various factors, including prior infection early in life (the geriatric population represents the largest reservoir of TB infection, particularly in developed nations),(7) immunosenescence, malnutrition, poverty, decreased access to health services and coexisting medical diseases.(8,9) The ageing population in Singapore is a phenomenon that will persist due to the country’s decreasing birth rates and increasing life expectancy. Given that TB incidence rates are higher among the elderly, there is a need to step up efforts to manage this vulnerable population. This can be done by increasing vigilance, promoting awareness and having a high index of suspicion for unusual, nonspecific clinical and radiological presentations.(10-14) These measures can facilitate early diagnosis and appropriate treatment, thereby minimising transmission of this infectious disease, and reducing its morbidity and mortality.
While extrapulmonary TB accounted for 14% of all TB cases in Singapore,(2) we found a consistently higher percentage (27.1%) of extrapulmonary TB among all the cases notified at SGH. This higher percentage could be explained by the hospital’s patient case mix; 9.9% of the patients with extrapulmonary TB were immunocompromised, nearly half from HIV, which predisposes them to the development of extrapulmonary TB.
With respect to HIV testing in patients newly diagnosed with TB,(15) we found that there was better adherence to published guidelines, in that an upward trend in HIV testing, from 43.8% in 2006 to 64.2% in 2010 was observed (
In the present study, the overall mortality rate throughout the five years remained constant at 12.0%. Death was mainly due to cancer, ischaemic heart disease and infections other than TB. Among the 28 (1.4%) patients who died from TB, 75.0% were smear-positive and 22 (78.6%) patients were diagnosed on their first presentation to the hospital, suggesting that medical attention was sought very late in the course of illness. Increasing public awareness of the signs and symptoms of TB and encouraging early medical consultation may improve TB mortality rates. The remaining six patients had delayed TB diagnosis due to confounding medical illnesses. Thus, as we endeavour to minimise mortality, there is also a need to heighten our index of suspicion of TB, so that expedient diagnosis and treatment can be delivered.
To conclude, TB continues to result in significant morbidity and mortality in Singapore, and thus, there is no room for complacency in our fight against this infectious disease. Efforts should be concentrated on the elderly population, as this vulnerable group is at a high risk of developing TB.